The blogs vs. Case-Deaton

But most of the critics have overstated their case pretty severely here. The Case-Deaton result is not bunk - it's a real and striking finding.
Harris and Geronimus' Critique
Harris and Geronimus' Critique
First, let's talk about the most popular critique - Malcolm Harris' post in the Pacific Standard. Josh Zumbrun of the Wall St. Journal had a good counter-takedown of this one on Twitter.
Harris notes that the Case-Deaton paper hasn't gone through peer review, but fails to note that the 2015 paper, which said basically the same thing, did go through peer review.
Harris notes that the Case-Deaton paper hasn't gone through peer review, but fails to note that the 2015 paper, which said basically the same thing, did go through peer review.
Harris also takes issue with the labeling of non-college-graduates as "working class", but this is a journalistic convention - Case and Deaton themselves use the term "working class" twice in their paper, but only when talking about possible economic explanations for the mortality increase. At no point do they equate "working class" with an educational category; that is entirely something that writers and journalists (including myself) do.
And personally speaking, who really constitutes the "working class" seems like one of those internecine Marxist debates best left in the 1970s. When I use the term to mean "people without a college degree", I specify that that's what I'm talking about.
But Harris' central critique is that, according to him, Case and Deaton have ignored selection effects. Obviously, if more people graduate college, there's a composition effect on the ones who still don't graduate. If mortality goes down by education level, this composition effect (which Harris calls "lagged selection bias") will raise non-college mortality even if mortality rates aren't changing at all. There's a 2015 paper by John Bound et al. (which Case & Deaton cite) showing that once these selection effects are taken into account, there's "little evidence that survival probabilities declined dramatically" for the lowest education quartile. Harris heavily cites Arline Geronimus, one of Bound's co-authors, who makes a number of disparaging comments about Case & Deaton's papers.
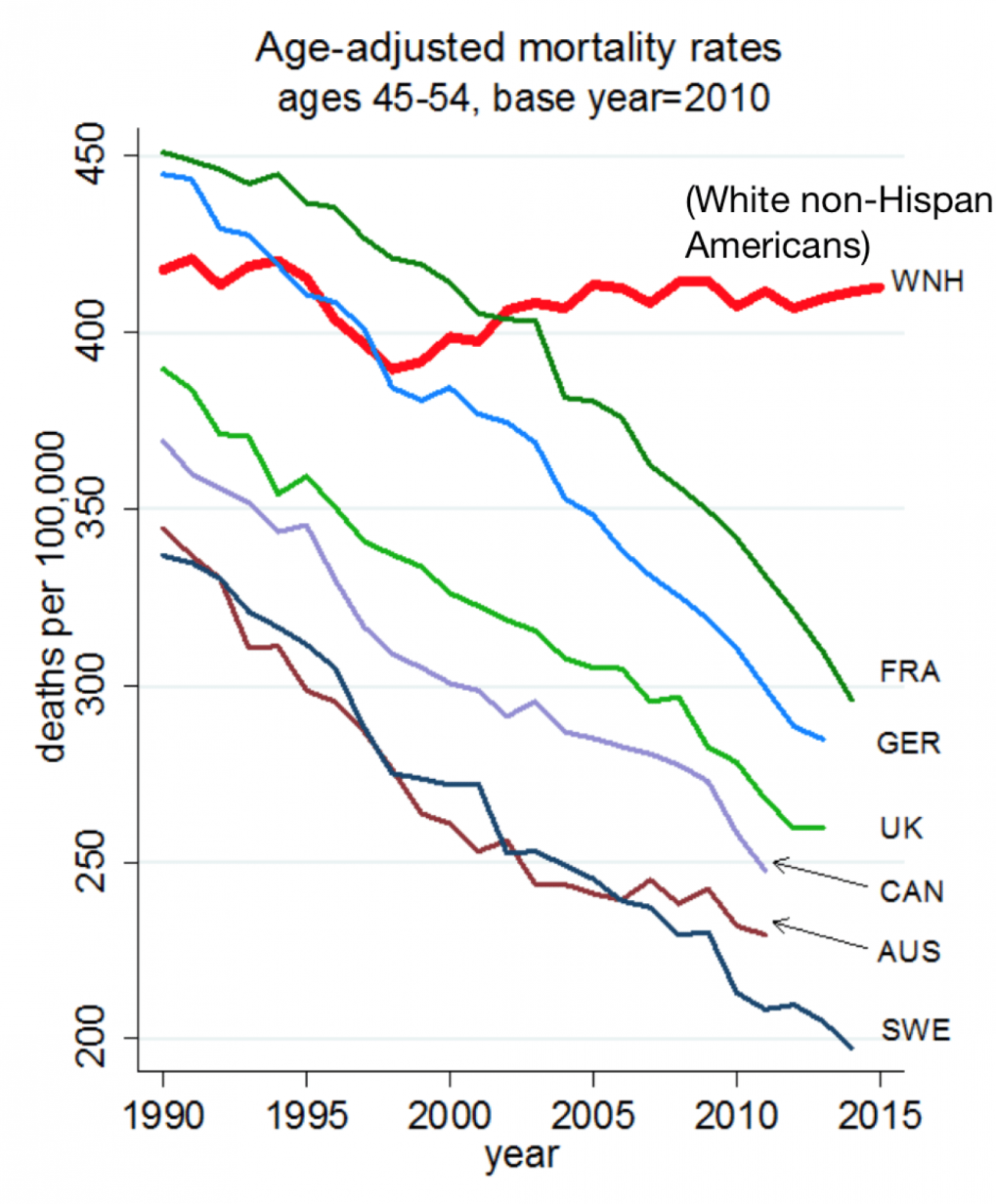
Selection effects are very real (and John Bound is one of the best empirical economists out there). Attrition from the non-college group is important. But as Zumbrun points out, once you lump all white Americans together - which totally eliminates the education selection effect - the mortality increase remains. Just look at this graph from the 2015 paper:

USW is all U.S. whites age 45-54, independent of education. USH is U.S. Hispanics. The rest are other countries - France, Germany, the UK, Canada, Australia, and Sweden. An age-adjusted graph from the more recent paper (which takes into account aging within this group) looks the same.
This graph shows two striking things. First, around 2000, the trend for middle-aged U.S. whites - all educational groups combined - stopped going down and started going up. Bound et al. might not say that qualifies as a "dramatic" increase, but it is clearly an increase, and that fact has nothing to do with education selection effects.
Second, and even more importantly, the USW trend post-2000 is markedly, hugely different from the trends for all other countries AND all other racial groups (though U.S. blacks are not displayed on the graph for some reason, Case & Deaton report that their mortality rates have also been trending downward).
This trend difference is far more important than the absolute change in mortality. It means that while good things are happening throughout the developed world that are causing mortality to fall for almost everyone, U.S. whites are being left out of this trend. Geronimus, Harris, and other critics spill a lot of ink over whether the USW trend is really upward or flat, but this distracts from the real issue, which is the big difference between U.S. whites and everyone else in the developed world.
In my opinion, if Case & Deaton made a mistake, it was to put too much emphasis on education, and not enough emphasis on this stark difference in international and racial trends.
Gelman and Auerbach's Critique
Gelman and Auerbach's Critique
OK, so let's get to Gelman's critique. Whereas Harris and Geronimus are essentially criticizing Case & Deaton for disaggregating the data too much by education level, Gelman & Auerbach are criticizing them for aggregating the data too much by race. Gelman & Auerbach have created an enormous database of mortality graphs for Americans of every conceivable combination of race, age, gender and geographical location. They find that there's considerable heterogeneity within U.S. whites - for some subgroups, mortality has been falling.
That's interesting and cool. But it doesn't invalidate the result, as Slate's overzealous headline writer seems to think. Disaggregating just gives us clues for where to look to explain the main result.
Disaggregation also distracts from the key issue of trend comparison. Gelman & Auerbach, like Harris, and like Bound et al., focus on whether the U.S. white mortality trend - or the trend for this or that subgroup of U.S. whites - is rising, falling, or flat. But the key takeaway from Case & Deaton's research is that U.S. whites aren't sharing in the mortality decline that U.S. nonwhites and Europeans are all enjoying. Gelman & Auerbach don't display any data for European countries, and they don't display demographically matched U.S. whites and nonwhites on the same graphs, making it hard or impossible to do the kind of visual trend comparison that is so easy to do in the Case-Deaton graph above.
Ironically, at the end of their Slate article, Gelman & Auerbach make a statement that relies heavily on exactly the type of aggregation that they criticize Case & Deaton for doing:
Of course, there is one simple story the data does seem to confirm: Minorities still have significantly higher fatality rates than white Americans. But that’s not news.
That might or might not still be true if you add up all U.S. minorities. But for Hispanics, it's false, and has been false for many years. Here's a Case-Deaton's graph for one age cut that illustrates the point. Compare the line for "White non-Hispanics (all)" to the line for "Hispanics":

It's also not true for Asian-Americans. Both Asians and Hispanics have lower mortality than their white counterparts. So by saying "minorities still have significantly higher fatality rates than white Americans", Gelman & Auerbach are rather hilariously failing to disaggregate. (From a quick look at CDC data, they also might just be plain wrong).
Why All The Critiques?
Why All The Critiques?
So why are people tripping over themselves to launch attacks on Case & Deaton? It's pretty obviously politics. Here are some excerpts from Harris' post:
[Some] have suggested that the Dems have to renew their focus on white working-class men if they want to win. In this view, liberals have become distracted by so-called “identity” issues like feminism, Black Lives Matter, transgender bathroom access, and the musical Hamilton, thus alienating the underserved voters Donald Trump was then able to nab. Underlying this argument is a series of reports on the immiseration of the white working class and its members’ increasing tendency to die...
[H]ow will this report be understood? I’d wager it’s something like the Brookings blog headline: “Working Class White Americans Are Now Dying in Middle Age at Faster Rates Than Minority Groups.” I asked Geronimus if that was, to her understanding, a true statement: “I think that’s misleading, I really do. Oh boy,” she laughs, “there’s so much wrong with that. That headline makes it sound like problems are worse for white Americans than black Americans.” The narrative is wrong, but it’s not the first time Geronimus has heard it since the election. The Case and Deaton paper, she says, fits conveniently in this story, and it’s one she fears Americans are primed to believe...
In [Case and Deaton's] graphs, white lives literally count more, and black lives less. But whether in health, income, wealth, or educational attainment, American white privilege is still very much in effect, and no statistical tomfoolery can change that.
In any case, it's clear that a lot of the eagerness to trash Case & Deaton's results comes from political reasons.
Is focusing on increasing white mortality a way to preserve white privilege and ignore the problems of black Americans? Maybe. I don't know. Personally, I'd think results like Case & Deaton's would help convince white Americans that the problems of black America aren't due to any unique pathology of black culture, and that white and black Americans are in the same boat together. I'd think it would be a powerful corrective to the poisonous Republican narrative that only black Americans need government help. But again, I'm no expert on how data will get used to create narratives (and I'm not sure anyone is an expert on that).
But anyway, the critiques of Case-Deaton are overdone. Maybe Case & Deaton should have focused less on disaggregating by education, and more on disaggregating by gender, age, and region. But those are quibbles. The main results are real and important.
Update 1 - More About Selection Effects
A couple people, after reading this post, asked me "OK, but did Case & Deaton ignore the selection effect, or not?". The answer is: They certainly didn't make any dumb mistakes. They intentionally ignored it, and they had their reasons. But it really doesn't matter, because I think the whole education issue is far less important than the key result.
Let me explain.
Case & Deaton obviously knew about the selection effect. They cited and explained Bound et al.'s paper, and they also mention the selection effect later in their own paper. But they intentionally don't try to take it into account.
Why not? Well, suppose you think of education as a drug that prevents mortality - kind of like statins. Case & Deaton seem to think of it this way. Now suppose that in 1990, 50% of people take statins, and in 2010, 75% of people take statins. And you observe that for the cross-section of people who don't take statins, mortality increased from 1990-2010.
There's obviously a selection effect here. The people who shifted from not taking statins to taking statins between 1990 and 2010 were probably richer than those who didn't make the shift - and, hence, likelier to have healthier lifestyles. So some of the increase in mortality among the "doesn't take statins" group will come from the changing composition of this shrinking group. That's the selection effect.
But does that mean you should correct for this bias by making sure your comparison groups represent 50 percent of the population in both 1990 and 2010? That's like what Bound et al. do. But that will mean putting some statin-takers in with the "no statins" people in 2010! Suppose you do this, and you find that once you do this, mortality for the "lower statin-taking" half of the population remains unchanged between 1990 and 2010. You say "Whew, once we control for selection effects, the lower-statin group didn't actually see a rise in mortality."
But a lot more of the people in that "lower" group take statins in 2010 than in 1990! In your effort to control for composition effects, you've forced yourself to ignore some of the beneficial effect of statins. If they hadn't started taking statins, their mortality probably would've gone up instead of staying constant!
Which method is right? Should you ignore composition effects, or partially ignore treatment effects? It depends on what you think is important, the treatment effect or the overall outcome. Bound et al. think the overall outcome is important, so they use percentiles. Case & Deaton think the treatment effect is important, so they use statin...er, education groups.
And what I'm saying in the post above is that I think neither of these things is really that important compared to the main finding, which is the trend comparison. I'm saying "Who cares? All those French and German and British and Canadian and Australian and Hispanic-American people over there are getting a lot fewer heart attacks, statins or no statins!" The trend comparison, I believe, is the big takeaway from the Case-Deaton paper, and the education issue is a bit of a sideshow.
Hopefully that clears that up.
Update 2 - Age Adjustment
In the comments, Andrew Gelman brings up age adjustment. I mentioned that earlier, but just so you can see, here are the age-adjusted and non-age-adjusted versions of the Case-Deaton mortality comparison charts:


Update 1 - More About Selection Effects
A couple people, after reading this post, asked me "OK, but did Case & Deaton ignore the selection effect, or not?". The answer is: They certainly didn't make any dumb mistakes. They intentionally ignored it, and they had their reasons. But it really doesn't matter, because I think the whole education issue is far less important than the key result.
Let me explain.
Case & Deaton obviously knew about the selection effect. They cited and explained Bound et al.'s paper, and they also mention the selection effect later in their own paper. But they intentionally don't try to take it into account.
Why not? Well, suppose you think of education as a drug that prevents mortality - kind of like statins. Case & Deaton seem to think of it this way. Now suppose that in 1990, 50% of people take statins, and in 2010, 75% of people take statins. And you observe that for the cross-section of people who don't take statins, mortality increased from 1990-2010.
There's obviously a selection effect here. The people who shifted from not taking statins to taking statins between 1990 and 2010 were probably richer than those who didn't make the shift - and, hence, likelier to have healthier lifestyles. So some of the increase in mortality among the "doesn't take statins" group will come from the changing composition of this shrinking group. That's the selection effect.
But does that mean you should correct for this bias by making sure your comparison groups represent 50 percent of the population in both 1990 and 2010? That's like what Bound et al. do. But that will mean putting some statin-takers in with the "no statins" people in 2010! Suppose you do this, and you find that once you do this, mortality for the "lower statin-taking" half of the population remains unchanged between 1990 and 2010. You say "Whew, once we control for selection effects, the lower-statin group didn't actually see a rise in mortality."
But a lot more of the people in that "lower" group take statins in 2010 than in 1990! In your effort to control for composition effects, you've forced yourself to ignore some of the beneficial effect of statins. If they hadn't started taking statins, their mortality probably would've gone up instead of staying constant!
Which method is right? Should you ignore composition effects, or partially ignore treatment effects? It depends on what you think is important, the treatment effect or the overall outcome. Bound et al. think the overall outcome is important, so they use percentiles. Case & Deaton think the treatment effect is important, so they use statin...er, education groups.
And what I'm saying in the post above is that I think neither of these things is really that important compared to the main finding, which is the trend comparison. I'm saying "Who cares? All those French and German and British and Canadian and Australian and Hispanic-American people over there are getting a lot fewer heart attacks, statins or no statins!" The trend comparison, I believe, is the big takeaway from the Case-Deaton paper, and the education issue is a bit of a sideshow.
Hopefully that clears that up.
Update 2 - Age Adjustment
In the comments, Andrew Gelman brings up age adjustment. I mentioned that earlier, but just so you can see, here are the age-adjusted and non-age-adjusted versions of the Case-Deaton mortality comparison charts:

Can you see a difference?? The red trend line, for U.S. whites, looks almost the same, while every other trend line still falls steadily and dramatically.
In fact, adjusting for age makes the comparison with European countries - i.e., what I think is the central result of the paper - even more stark. It also illustrates why obsessing over whether the red line goes a little bit up, a little bit down, or stays flat is a total distraction - the real point is that every other trend line goes strongly down. (Annoyingly, U.S. Hispanics aren't on the age-adjusted chart, but you can see it's not going to make much difference.)
Update 3 - Dual Y-Axis Graphs
Earlier, I made fun of Harris for saying that "white lives literally count more" than black lives in a Case-Deaton graph. But a commenter explained what Harris meant - he was complaining about dual y-axes. Here's the graph in question:

Harris is actually right - the y-axis for black mortality is much more compressed than the y-axis for white mortality. Because of dual y-axes, white lives do literally count for more. This is, indeed, a crappy graph.
BUT, it's a crappy graph because it massively understates the size of the black mortality decline. If the y-axes had the same scale, you'd see a blue line (for white mortality) that stayed just about flat, and a red line (for black mortality) that zoomed downward. In other words, making white lives count the same as black lives on this graph would show black people doing a lot better than they were before, and white people not doing a lot better than they were before. That seems like exactly the message that Harris doesn't want to send. So I'm not quite sure why Harris is complaining. Anyway, the big takeaway from this graph is: Don't make dual y-axis graphs.



{kind=link}
Comments
Post a Comment